Can the depletion of B-cells—the primary drivers of the body’s humoral immune response—compromise the effectiveness of modern immunotherapy in treating liver cancer?
For patients with inoperable hepatocellular carcinoma (HCC), immune checkpoint inhibitors (ICI) have become a standard of care. These therapies do not attack the cancer directly; instead, they remove the molecular brakes that prevent the immune system from recognizing and destroying malignant cells. While the primary mechanism involves the activation of cytotoxic T-cells, there is increasing discussion regarding whether humoral immune mechanisms, mediated by B-cells, also contribute to the success of these treatments.
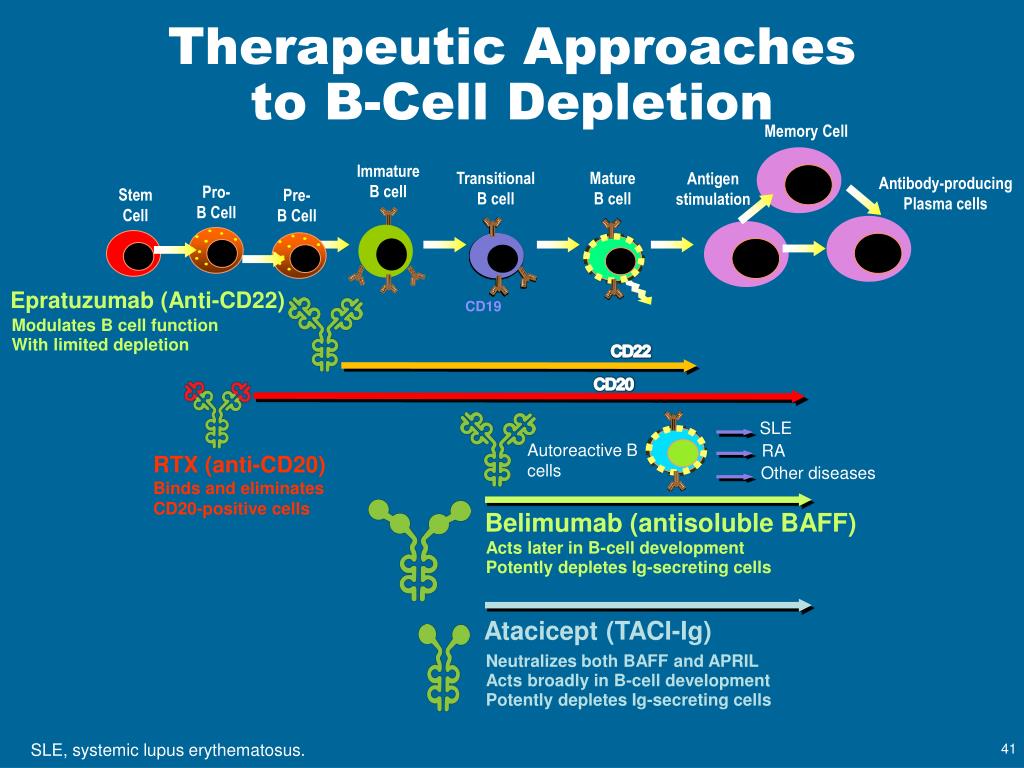
This consideration is particularly relevant for patients who have previously undergone therapy for lymphomas using agents like Rituximab, which results in a significant reduction in their B-cell population. Because B-cells are responsible for producing antibodies, their absence—known as B-cell depletion—could theoretically influence the immune system’s ability to respond to checkpoint inhibition.
The tension between cellular and humoral immunity
To understand the relationship between these mechanisms, it is necessary to distinguish between the two main arms of the adaptive immune system. Cellular immunity relies on T-cells to identify and kill infected or cancerous cells. Humoral immunity, conversely, relies on B-cells to produce antibodies that neutralize pathogens or mark targets for destruction.
Immune checkpoint inhibitors are designed to amplify the cellular response. By blocking proteins such as PD-1 or CTLA-4, ICIs allow T-cells to regain their potency. However, researchers have questioned whether B-cell depletion can influence the overall effectiveness of this process and whether T-cells can achieve a full clinical response independently.
Rituximab complicates this picture. As a monoclonal antibody targeting the CD20 protein found on the surface of B-cells, Rituximab is highly effective at clearing these cells from the system to treat certain blood cancers. If the humoral response is a prerequisite for ICI efficacy, a patient who has received Rituximab would, in theory, be less likely to respond to immunotherapy for a subsequent cancer, such as HCC.
Complete remission despite B-cell loss
A recent report from medonline.at provides a counter-narrative to the theory that B-cells are indispensable for ICI success. The report describes a specific clinical case involving a patient who had previously undergone lymphoma therapy, resulting in pronounced B-cell depletion.
Following this prior treatment, the patient was diagnosed with inoperable hepatocellular carcinoma. Despite the lack of a robust B-cell population, the patient was treated with immune checkpoint inhibitors. The outcome was a complete remission of the HCC.
This observation is significant because it demonstrates that the absence of a humoral immune response did not preclude a total therapeutic victory over the liver cancer. The case suggests that the activation of cytotoxic T-cells via ICI can be sufficient to drive a complete response, even when the B-cell arm of the immune system is largely inactive.
Implications for complex patient histories
While a single case cannot establish a universal rule, it offers a critical data point for clinicians treating patients with comorbid conditions or prior immunotherapy histories. The interaction between previous B-cell depleting therapies and current ICI protocols remains an area of clinical interest regarding how these factors impact overall efficacy.
The medonline.at report highlights that in this specific instance, a history of Rituximab use and the resulting B-cell depletion did not prevent the patient from achieving a positive clinical outcome. This suggests that the immunologic profile of a patient, specifically the absence of B-cells, may not be an absolute barrier to the success of ICI therapy.
The primary implication is that the cellular immune response, once unleashed by checkpoint inhibitors, may possess enough autonomy to eradicate inoperable HCC without the supporting infrastructure of the humoral system. This case demonstrates that complete remission is possible even in the context of profound B-cell depletion.